Sign up for the daily CJR newsletter.
The Wall Street Journal editorial board’s Joseph Rago makes a whopper of an error in a column Tuesday extolling Paul Ryan’s plan to turn Medicare into a voucher program that probably wouldn’t cover the cost of old folks’ health care.
Under the 2008 roadmap, seniors would get a straight cash voucher for $9,500 a year (the amount Medicare then spent per person), indexed to a blended measure of general inflation and the rise of health costs…
The 2012 budget, renamed the Path to Prosperity, indexed the payments to general inflation, starting at $15,000 (the amount Medicare now spends per person).
Wow. Medicare costs per recipient have jumped 58 percent in four years in a depressed economy? We’re doomed!
Fortunately, these numbers are just wrong. Medicare spent $10,945 per beneficiary in 2008 and projects spending $12,351 per person this year, according to its trustees:
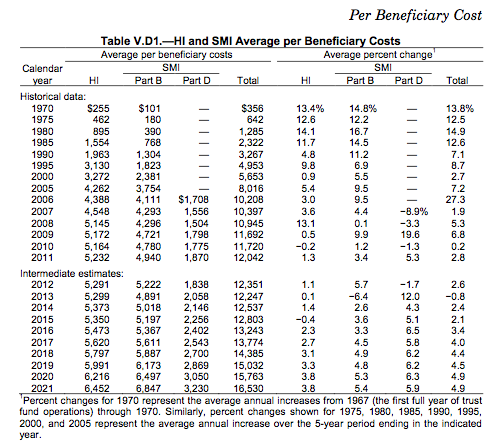
That’s a 13 percent increase, or 6 percent in real terms. Too high, yes, but far from the WSJ’s apocalyptic numbers, and quite a bit less than private-sector costs, which jumped 19 percent from 2008 through last year, nearly twice the growth rate of Medicare’s costs.
So what’s with that $15,000 number? That’s what the Congressional Budget Office projects Ryan’s plan would cost Medicare per beneficiary in 2022, not 2012. That $9,500 was what Ryan pitched for 2009. Big difference.
Those numbers aren’t all that’s misleading here. Here’s Rago implying that Bill Clinton supported premium support/vouchers:
President Clinton’s 17-member Medicare commission, chaired by Louisiana Democrat John Breaux, endorsed the reform in 1999.
But it wasn’t Clinton’s commission, it was a bipartisan one formed by a law passed by the Republican Congress and signed by Clinton. You might as well call it the Gingrich commission. Clinton appointed just four of its 17 members, as many as Gingrich, and all four of them voted against it. Clinton himself immediately rejected the majority’s findings, and the commission itself, far from “endorsing” anything, deadlocked one vote short of the required 11 to approve a report. Or as the WSJ news pages put it back in 1999, “the 17-member Medicare commission met for the final time and failed, by a single vote, to endorse the plan as a formal recommendation to Congress and the White House.”
FactCheck.org was on this back in May of last year, responding to a Paul Ryan claim cribbed from the WSJ edit page, apparently (his office sent out a 2010 WSJ editorial making the claim as a press release), about the commission and premium support.
But any attempt to cast the 1999 report as bipartisan or suggest it was Clinton’s commission is misleading.
The Journal editorial page has done so at least eight times in the last two years in a bid to suggest that privatizing Medicare had more Democratic support than it ever actually did. First reader to prove to me that WSJ is genuinely interested in Bill Clinton’s thoughts on vouchers gets a complete set of Whitewater: From the Editorial Pages of the Wall Street Journal Vols. 1-5.
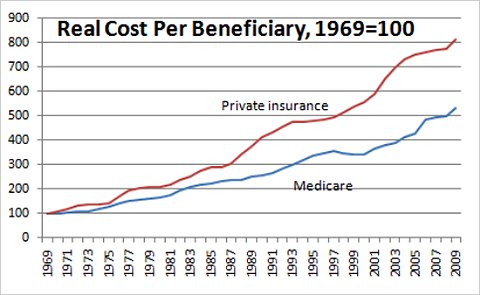
Anyway, the faster rise in private health costs means you have to have a certain amount of cognitive dissonance to claim, as Ryan and the WSJ do, that shifting health-care spending into the private sector would curb medical inflation. Here’s a Paul Krugman chart that shows how much faster private health care costs have risen compared to government-run Medicare’s:
Has America ever needed a media defender more than now? Help us by joining CJR today.